
Tackling Mitochondrial Dysfunction
Tackling Mitochondrial Dysfunction
Opportunity

Bandaid approaches that treat symptoms and fail to address root causes of illness, leave patients on a never ending treadmill. Opportunities to treat the causes of Long COVID and many mitochondrial age-related illnesses are being lost.
Mitochondrial disorders come in two broad categories, Primary and Secondary. Both involve genetic mutations, however from different sources.
In medical school, many programs have traditionally focused attention on primary mitochondrial diseases. These are illnesses associated with inborn genetic traits that result in functional failures of one or more of the mitochondrial roles.
Aging, viral infections (like COVID-19), diet and various environmental exposures can contribute to Secondary Mitochondrial Disorders. Inflammation from these or other causes can result in mutations to mitochondrial (mtDNA).

Complicated, yes. But herein lies opportunity. Because there are many mitochondria in each cell, mutations happen unevenly. Some mitochondria can maintain optimal function, while others may not.
Under the right conditions, mitochondria are self-repairing organelles through the process of biogenesis. And, under favorable conditions, the process favors mitochondria that are functional.
Although the symptoms and organs may differ, mitochondrial dysfunction (MD) is shared by Long COVID and many age-related diseases. Dementia, diabetes, a variety of neurological and cardiovascular diseases, sarcopenia (loss of muscle mass and strength), exercise intolerance, fatigue and more involve MD. MD and related disorders of metabolism, limit the capacity of cells to produce energy and to conduct other vital mitochondrial functions.
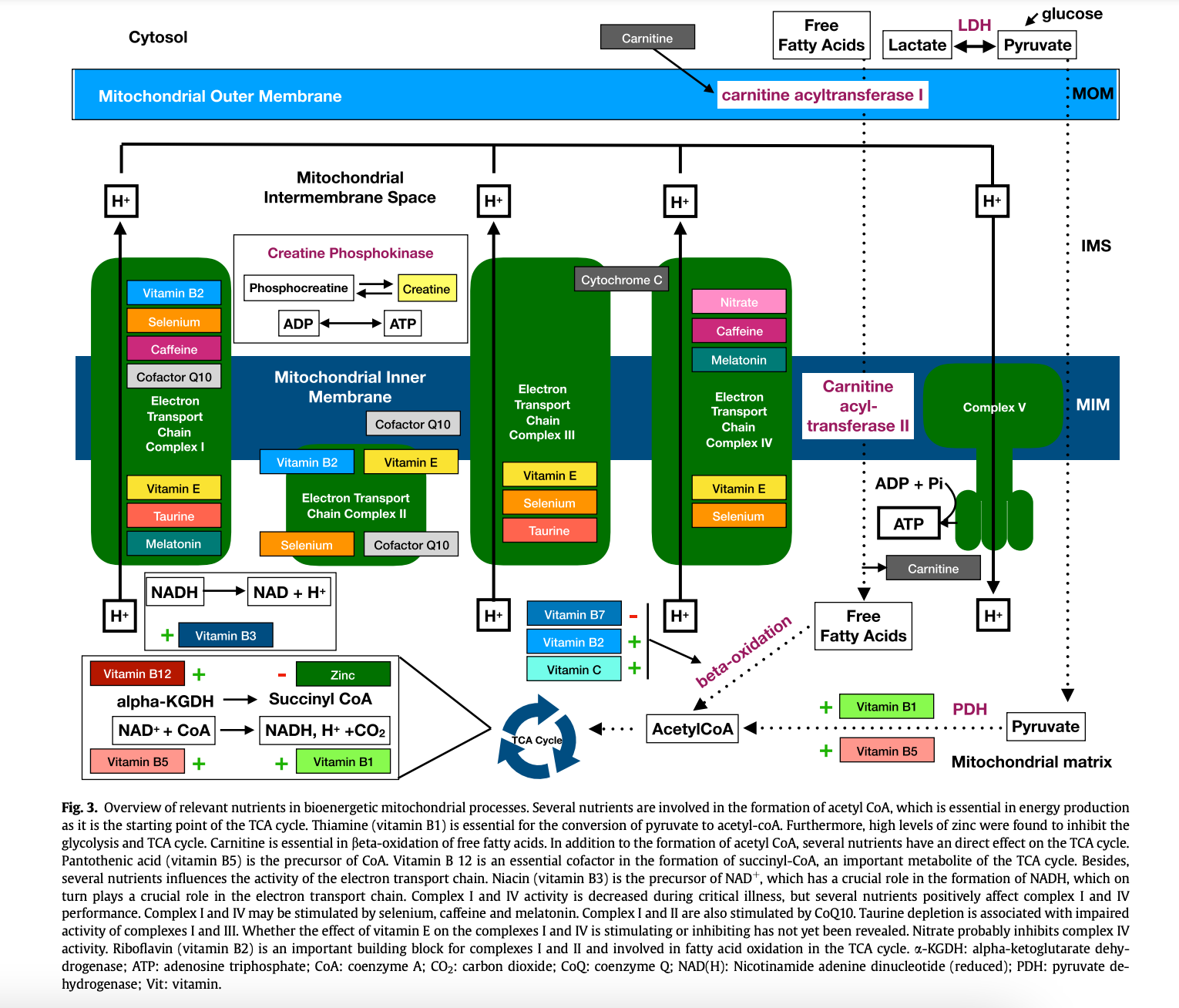
A rationale for developing treatment protocols for patients with secondary mitochondrial dysfunction was set out in 2017. It was needed to address MD in critically ill patients. Interestingly, since mitochondria have intense nutritional needs, the authors focused on which vitamins, minerals and amino acids are needed for optimal function.
From the perspective of both patients and providers, addressing MD as an integrated part of treating many of the above mentioned disorders would provide timely help for those burdened by disease. Clearly, this would be a better option than limiting care to the treatment of symptoms.
Sadly, the current CDC “goal of medical management of Long COVID is to optimize function and quality of life through established symptom management approaches.”
I was hopeful that searching the CDC site for professional geriatric care guidelines would point to relevant and meaningful actionable recommendations. Yet, there seems to be no consideration of the Big Picture. Guidance is organized primarily by disease. Healthy aging is found with materials on dementia.
These are not small problems. Currently, 18% of the U.S. population, is 65 years of age or older. Worldwide, seniors account for about 10% of the population. This relatively smaller segment of the population accounted for approximately 37 percent of all healthcare spending in the U.S..
Reportedly Long COVID has impacted middle-age individuals more than seniors. In the U.S. 6.4% of non-institutionalized adults are reported to have experienced Long COVID. The number is likely much higher. The costs in the U.S. of Long COVID alone, is being estimated in the trillions of dollars. This includes healthcare as well as lost wages and reduced productivity.
It’s not as if we are not devoting resources to healthcare. In 2022 U.S. health-spending accounted for 17.3 percent of the nation's Gross Domestic Product, reaching $4.5 trillion. I suspect that treating MD could reduce health care needs and spending.
The U.S. has the highest health care costs per capita of any country in the world. We should be getting more for our investment in healthcare. Isn’t it time for a paradigm shift?
I’d like to leave you with illustrations from two articles that graphically layout the biology of nutritional opportunity in caring for the older generation and those with various acute and chronic diseases associated with MD.
Feeding Mitochondria: Potential role of nutritional components to improve critical illness convalescence lays out considerable detail of the mechanics of mitochondria including what they are thought to need to function optimally. I recommend this paper for those who want to build a better understanding of the science.
As we age, our nutritional needs change. The authors of Can Nutrition Contribute to a Reduction in Sarcopenia, Frailty, and Comorbidities in a Super-Aged Society? take a broader view of nutritional needs and opportunities in a variety of diseases that impact older adults.
Note that in the figure below they show which nutrients have been demonstrated to help prevent disease. In the lower half, they include nutrients that have value in treatment of the various diseases.
Both of these articles are Open Access and should be available to you.

Another easy to read reference, Mitochondria and the Future of Medicine was recently reviewed as part of this series. Author, Dr. Lee Know does a credible job laying out the complexity of dealing with mitochondrial associated diseases including the nutritional details essential to keep them working.
For those looking for more in-depth discussions, I offer zoom sessions to those who subscribe at the Founding Member level. I also do my best to respond to questions in the comments section for all subscribers. Many thanks to all for your support.
Mardi,
I am not medically trained but read and listen to lectures on the topic of Long Covid. You paint a picture of recovery like few do...insightful, logical, and totally helpful. I look forward to reading
your regular posts. More doctors should be updating their knowledge on MD.
Thank you,
Jane
This is a very important article! Thank you, Dr. Crane-Godreau!